Psoriasis
is a chronic inflammatory disease & also hyperproliferative skin disease.it is characterized by well defined ,erythematous scaly plaques ,particularly affecting extensor surfaces and scalp & usually follows a relapsing & remitting course .Psoriasis affects approximately 1.5 -3% of Caucasians .It affects both equally .
Aetiology & pathogenesis
The pathogenesis of psoriasis is multifocal and genetic and environmental factors are important.The genetic component is complex and polygenic .If one percent has psoriasis ,the chance of a child being affected is about 15 -20 %.If both parents have the disease,this rises to 50% and the risk is increased further if a sibling has the disease .Several genes such as the most replicated gene is PSORSI, located with in the MHC on Chromosome 6 & encoding an epidermal protein ,corneodesmosin.It is thought that this gene anomals for almost half of the heritability of Psoriasis .
Exacerbating Factors in psoriasis
- Trauma -Psoriatic lesions can appear at sites of skin trauma such as scratches or surgical wounds .
- Infection-Beta -haemolytic streptococcal throat infections often precede guttate psoriasis.
- Sunlight
- Drugs – Antimalarials ,Beta-blocker,NSAIDs,Anti -TNF-Alpha drugs
- Psychological factors
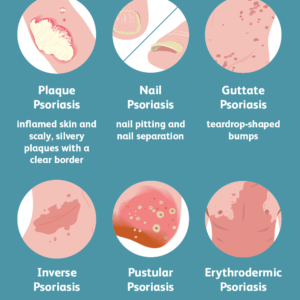
Clinical Features

Psoriasis has several different presentation & usually represents more stable disease .The typical lesion is a raised ,well demarcated erythematous plaque of variable size .In untreated disease silver or white scale is evident and more obvious on scraping the surface . The most common sites are the extensor surfaces ,notably elbows & knees & the lower back .Others include
- Scalp :Involvement is seen in approximately 60 % of patients ,typically easily palpable ,erythematous scaly plaques are evident with in hair bearing scalp margin .Occipital involvement is common and difficult to treat .Involvement of other sites “Seborrhoeic sites “such as eyebrows nasolabial and again may be confused with seborrhoeic dermatitis .Temporary hair loss can occur but permanent loss is unusual.
- Nails:Involvement is common with thimble pitting ,onycholycosis ,subungual hyperkeratosis and periungual involvement .
- Flexures : Psoriasis of the natal cleft and submammary and axillary folds is usually symmetrical.
- Palms :Psoriasis of the palms can be difficult to distinguish from ecxema
Treatment
- Topical agents : Emollients,Tars,Dithranol,Vit D agonits,Retinoids ,Corticosteroids
- Phototherapies :UV B,PUVA
- Systemic Agents : Retinoids ,immunosuppressants ,(e.g. methotrexate ,ciclosporin ,mycophenolate ),Immunomodulators ( fumaric acid esters ),Biological (Infliximale ,etanercept)
Dermatocare Bangladesh